
Dr. Syam Reddy, National Subspecialty Lead for Body Imaging at Radiology Partners (RP), discusses RP’s focus on delivering quality care and enhancing patient and client experiences while leading innovation in AI and technology.
Dr. Syam Reddy is the National Subspecialty Lead (NSL) for Body Imaging at RP. A body and breast radiologist and practice president at RP Chicago, he and his practice joined RP in 2014. He is the clinical chair at UChicago Medicine Ingalls Memorial and a member of several physician support boards, as well as a facilitator for coaching circles. He holds memberships in the Chicago Radiologic Society, Breast Imaging American College of Radiology (ACR) Data Science Institute, ACR CT colonoscopy committee, the ACR HR Commission, Society of Cardiovascular CT (SCCT) and Society of Cardiovascular MR (SCMR). Outside of work, Dr. Reddy enjoys spending time with family – traveling, playing tennis with his kids, and learning the cello.
We talked to Dr. Reddy about his role with RP’s Clinical Value Team as NSL for Body Imaging, RP’s commitment to quality and innovation, the role of collaboration and AI in advancing subspecialty practice, and his excitement about leveraging imaging technology like MosaicOS™.
What inspired you to be a radiologist?
The biggest reason is my mom was a radiologist. Towards the end of her career, teleradiology was becoming more common. She had this monstrous screen she would have to bring home, and I saw her read these head CTs that took forever to load. That inspired me to see the mix of computers and medicine and how they meld together to help the patient. The more I learned about it, I was drawn to the fact that it’s almost like looking at artwork, trying to decipher what’s going on and putting all the pieces together – you’re a little bit of a detective, too. I also like my hands in a little bit of everything, and I found radiology to be a field that really covers all the specialties to a great extent.
What drew you to body imaging as a subspecialty?
I like body imaging because it’s so integrated with everything – from ER to developing subspecialties. I also got involved with breast imaging quite a bit, so those are the two areas I focused on. I really enjoy learning, and in radiology, there are always new updates, information and trials.
Talk about your decision to join RP.
Our group was one of the earliest groups to join RP, way back in 2014. At the time, we were a fairly large group, with about 100 radiologists across four or five states. Our group landed with RP because of their focus on quality. RP’s mission to transform radiology includes improving quality, patient experience and client-side experience, which drew our attention. That’s exactly what we wanted. Being a physician who can be integrated and involved with that process is really meaningful.
Talk about the change and growth you’ve seen within RP since you joined in 2014.
Looking back, I think RP has positioned itself as a practice that’s ahead of the curve in several ways. We’re the ones helping the rural areas that can’t get help. We’re working with reimbursement issues to ensure physicians are getting reimbursed properly to maintain their practices. And we’re the practice that’s ahead of the curve when it comes to AI and technology. I see a lot of vendors coming out, but I don’t know how many are radiology-driven with the input that we have and the speed at which we are progressing. All of those really speak volumes about what we are doing, what we have done and where we’re going.
What was your path to serving on our Clinical Value Team as the National Subspecialty Lead (NSL) for Body Imaging?
I started out being on the subspecialty advisory board. After a couple years, our previous NSL decided to explore other opportunities and asked me if I wanted to get involved. I thought it was a good way to get further into the subspecialty. I was nervous at first, but it was fun to jump in and meet everybody in the body imaging group. I’ve really enjoyed meeting other people in the practice and seeing all the things that we’ve developed over the years. I think there’s so much more potential – just the vastness of radiology really needs guidance for all these subspecialty exams that we do. There’s so much information out there.
What has been the most rewarding aspect of your NSL work?
I think sometimes we can get somewhat siloed, even within our own groups. When we come together in our advisory boards and discuss topics like trauma, we’re all on the same page. Those conversations give us the chance to say, “We do that too,” “This is how we do it,” “This is a great idea,” or “Maybe we can tweak it this way.” That sharing of ideas is so powerful. It’s great knowing there are so many resources out there and different ways to connect with people. And then there’s the challenge of pulling information together in a concise way. There are so many books and articles, so you have to dig through information. We need to get to a point where everything is very concise and easy to access, because that’s the way of the future.
Talk about the “Rad to Rad” peer learning program. What is it and what’s the goal of it?
When we think of our residents and fellows, a lot of information today is short-form – quick snippets like a one- or two-minute video on YouTube or a one-pager. With that in mind, we created the “Rad to Rad” peer learning program. It’s simple: share a couple of images from an important case and highlight the most valuable points. It’s super easy, super quick and very high yield. That’s the kind of content people are seeing on social media when it comes to radiology cases. Our hope is that it draws the attention of residents and fellows – and also keeps all of us engaged. We’re all busy, but if we can take a minute or two to see a case that boosts our confidence or helps avoid a mistake, it’s worth it.
How do you and the Clinical Value Team come together to create “Rad to Rad” learnings?
All of us are exposed to different cases in our practice, and some of them stand out. For example, maybe it was a miss, or maybe it was a great catch. I think most of us have a process where we document that, whether it’s a teaching case or something else, and we’re all very passionate about our desire to showcase our subspecialty. Those are the kind of cases we present to each other in our board meeting when we’re working on this. It’s kind of a working meeting; we’ll share the case, and then people will bring up some pointers, verify if it looks accurate, etc. Being able to create that is rewarding by itself.
Why is a team like the Clinical Value Team so integral to the rapid technology changes?
We’re all racing to get our work done, but we need someone to pause and make sure we’re running in the right direction. Sometimes speed without guardrails or guidance can lead to chaos pretty quickly. RP’s Clinical Value Team provides a forum that allows us to still move fast, but in the right direction, and ensure we’re doing it safely for our patients and the radiologists. That is so important. Our radiology societies play a similar role by ensuring new information and literature reach radiologists, so the quality of practice is always improving. Medicine is changing so quickly, and so is technology.
How would you define a successful future?
It seems like there’s this ever-growing gap between the volumes of work and the supply of radiologists. One of the things we’re focusing on is AI and how we can integrate it with radiologists to improve the whole process. To me, success would be all of that coming to fruition: leveraging AI while maintaining our quality and improving patient care. If we’re able to see all those things happen, that’s true success – no question.
You are an early user of Mosaic Clinical Technologies™. What has your experience been so far?
My background is in biomedical engineering, and the biggest decision I had to make was whether to go into computers or medicine. The reason I didn’t go into computers is that I tend to obsess about trying to get things right. That’s why I enjoy working with MosaicOS™ – I like creating and understanding. It’s very early, but the concept of telling AI to handle tasks like calculating volumes or percent changes is just incredible. I used to do all of that manually with a calculator. What I really want to know is how far I can push the envelope. There are people who know more than I do, and I’m excited to learn from them. I think we’re headed in the right direction, and it’s going to be pretty amazing.
How would you like AI to help support your specialty?
I’ve always felt the purpose of RP’s Clinical Value Team is to make it easier to practice in our subspecialty: being faster, more efficient and with high-quality content. As we become more subspecialized, our subspecialized referrers expect very specific content. If we can increase everyone’s skill set in that way, then I think we’re successful. There’s a shortage of body imaging radiologists and breast imaging radiologists; how do we use AI and the clinical value we provide to decrease the gap while increasing the number of people who are able to perform?
Dr. Syam Reddy earned his medical degree from the University of Illinois Medical Center in Chicago; completed his residency at Sparrow Health System; and completed his fellowship in body MRI imaging at Baylor College of Medicine in Houston.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned radiology practice in the U.S. Learn more about our mission, values and practice principles at RadPartners.com. For the latest news from RP, follow along on our blog and on X, LinkedIn, Instagram and YouTube. Interested in learning about career opportunities? Visit our careers page.




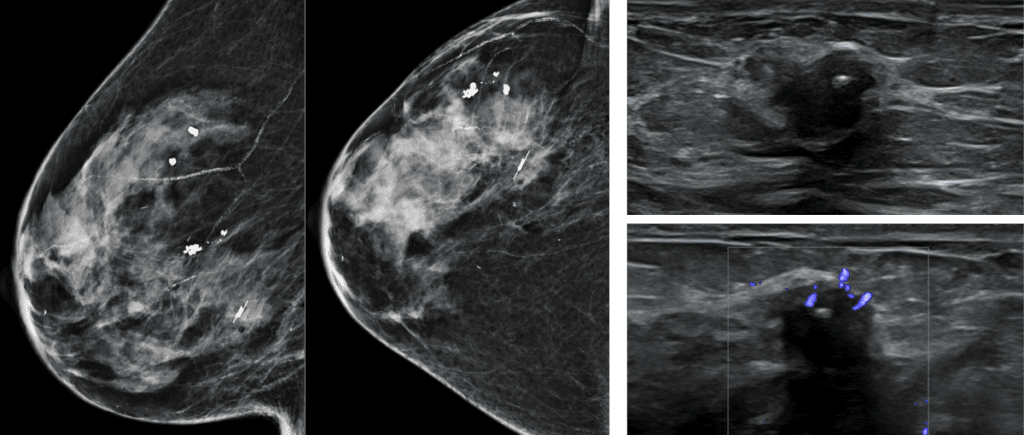 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.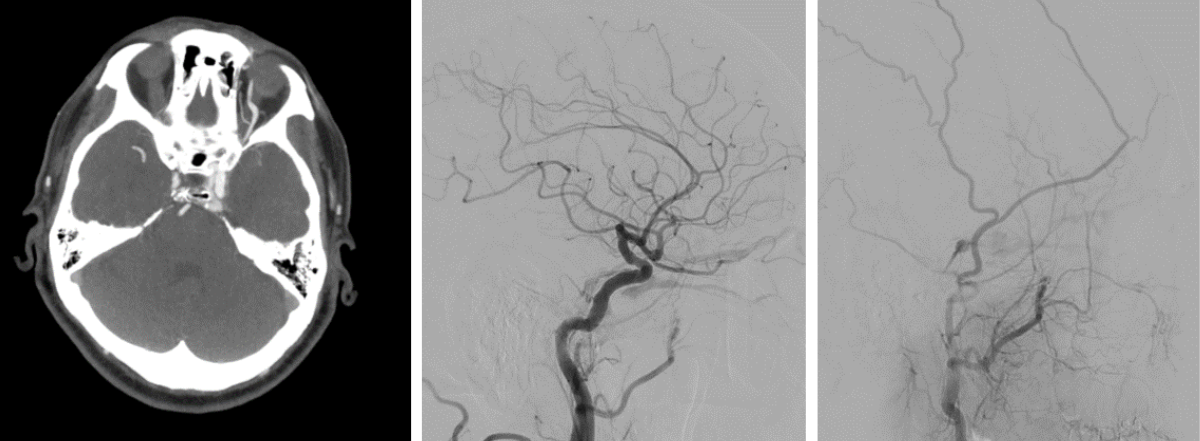 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.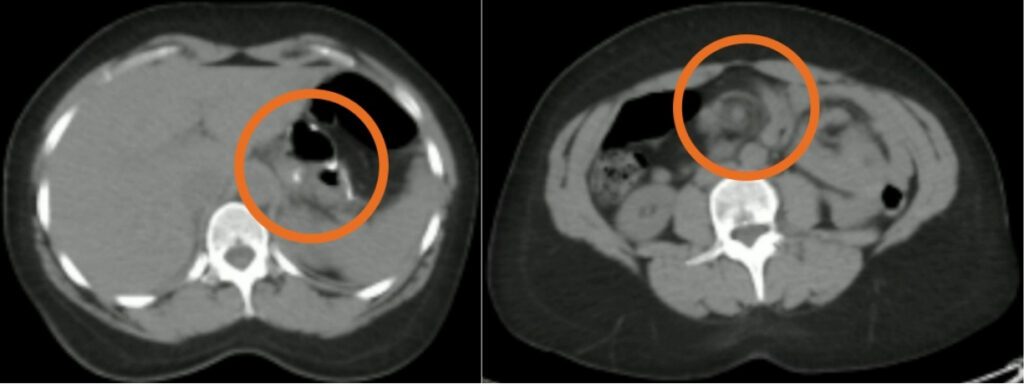 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived. Visit the
Visit the 