The Radiology Partners (RP) Interventional Radiology National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
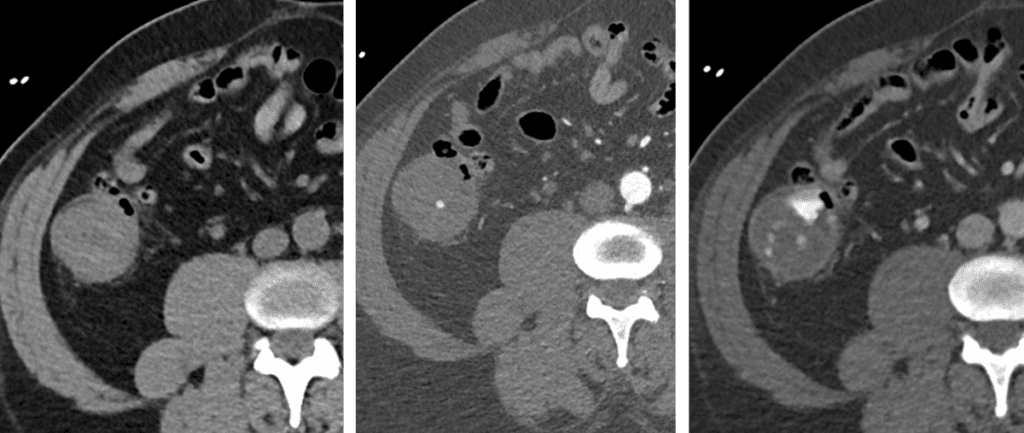
Higher specificity and anatomic localization of CTA enhances speed and accuracy of GI bleed diagnosis.
Active GI Bleed on CTA
Arterial extravasation that increases on delayed phase is diagnostic of active bleeding.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
CTA is exam of choice to diagnose acute GI bleeding – quickly replacing tagged RBC scans.
CTA protocol: No oral contrast, must include non con, arterial and venous phase imaging.
Non contrast imaging is key to avoid false positives.
Faster diagnosis = improved embolization success.
Multiphase CTA = Faster, more specific, better anatomic localization.
The Interventional Radiology National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Dr. Nina Kottler Named Chief Medical AI Officer of Mosaic Clinical Technologies™
Appointment underscores Mosaic’s role in advancing the next era of diagnostic imaging through clinical insight and intelligent technology
(NASHVILLE, Tenn.) Nov. 10, 2025 — Mosaic Clinical Technologies™ (Mosaic), the technology and AI services division of Radiology Partners (RP), today announced the promotion of Dr. Nina Kottler to Chief Medical AI Officer, effective January 1, 2026. Dr. Kottler previously served as Associate Chief Medical Officer of Clinical AI for RP, a role she has held since 2021, when RP established the Office of the Chief Medical Officer.
“Mosaic is accelerating our mission to transform radiology at a time when our specialty faces extraordinary demands,” Dr. Kottler said. “Radiologists are under more pressure than ever to do more with less without compromising accuracy or patient care. Capacity constraints and disconnected systems have impeded the radiology field’s ability to deliver care efficiently. Mosaic bridges that gap by connecting AI, clinical expertise and modern cloud technology into a single ecosystem that empowers radiologists with the right advanced tools, restoring focus to what matters most: delivering timely, high-quality care for patients.”
Dr. Kottler is a globally recognized expert and thought leader in the design and implementation of clinical AI at scale. In her new role, she will lead Mosaic’s clinical AI strategy, guiding the development and deployment of AI-native solutions that enhance diagnostic precision, optimize workflow efficiency and capacity and elevate the radiologist experience. Her leadership will be instrumental in shaping Mosaic’s clinical and technological direction, ensuring every innovation is grounded in real-world radiology practice and measurable patient impact.
“Dr. Kottler has been a driving force behind our clinical AI strategy from the start,” said Rich Whitney, Board Chair and CEO of Mosaic and RP. “Her visionary leadership, coupled with an unmatched ability to translate clinical needs into scalable, impactful technology, has already transformed how we think about and practice radiology. Under her guidance, Mosaic will accelerate our vision for the next era of radiology—one that fuses human expertise with intelligent technology to deliver better outcomes for patients, health systems and clinicians.”
Learn more about Mosaic Clinical Technologies™ and the many groundbreaking capabilities of MosaicOS™ during 2025 Radiological Society of North America (RSNA) held Nov. 30 – Dec. 4 at McCormick Place in Chicago.
North Hall #7108: Visit the RP and Mosaic booth to learn more about MosaicOS™, Mosaic’s proprietary, fully cloud- and AI-native operating system that seamlessly merges diagnostic technologies.
South Hall #1136: Connect with RP radiologists to learn what it’s like to practice with the leading, technology-enabled practice in the country.
About Mosaic Clinical Technologies™ and MosaicOS™
Mosaic Clinical Technologies™, the technology services division of Radiology Partners (RP), is powering the future of radiology through MosaicOS™—a proprietary imaging management platform designed to meet the specialty’s most pressing challenges. A fully cloud-native and AI-native operating system, MosaicOS™ is where innovation meets impact, seamlessly integrating diagnostic technologies, AI-powered tools and smart workflows into a single scalable solution. Mosaic Clinical Technologies™ supports RP’s national network of affiliated practices and commercial partners across the imaging landscape, redefining what is possible in enterprise imaging. Connect with us on LinkedIn.
About Radiology Partners
Radiology Partners, through its affiliated practices, is the leading technology-enabled radiology practice in the U.S., serving more than 3,400 hospitals and other healthcare facilities with high quality radiology, technology and artificial intelligence solutions. As a physician-led and physician-owned practice, our mission is to transform radiology by innovating across clinical value, technology, service and economics, while elevating the role of radiology and radiologists in healthcare. Using a proven healthcare services model, Radiology Partners provides consistent, high-quality care to patients, while delivering enhanced value to the hospitals, clinics, imaging centers and referring physicians we serve. Learn more at radpartners.com and connect with us on LinkedIn, X, Instagram and YouTube.
Why RP? A Q&A with Dr. Shaheen Hussaini, Pediatric Radiologist
Dr. Shaheen Hussaini discusses how Radiology Partners (RP) offers resources, support, collaboration and innovation to empower radiologists to make a meaningful impact on patient care and the future of radiology.
Dr. Shaheen Hussaini is the National Subspecialty Lead (NSL) for Pediatric Radiology at RP. A pediatric radiologist at Austin Radiological Association (ARA), she and her practice joined RP in 2019. She is a member of the American College of Radiology, Radiological Society of North America, Society of Pediatric Radiology and Texas Medical Association. Outside of work, she enjoys traveling and spending time with her husband and children, and she loves reading, hiking and trying new activities – often bringing her family along for the adventure.
We talked to Dr. Hussaini about her role as NSL for Pediatric Radiology and how RP offers radiologists a true seat at the table.
Tell us about why you chose radiology and, ultimately, pediatric radiology.
What interested me in radiology was how collaborative it is. You get to talk to a variety of physicians and sub-specialists and use those different perspectives to determine the best way to answer their questions about the patient. It’s also fun to play with toys – and radiology has a lot of toys. In pediatric radiology, you interact with patients who don’t have a voice; these are small patients often too young to explain what’s wrong. It helps that they’re cute, even when they’re angry at you because what you’re doing to them is not fun. Going through pediatric radiology training while pregnant and as a new parent helped me relate to the children and families in a much more personal way. It elicited a desire to help and play small part of their diagnostic and treatment journey, and I felt I could be more empathetic and understanding. Another thing I love about pediatric radiology is the variety, because there are all varying subspecialties that are part of pediatric radiology instead of focusing on just one area, such as neuroradiology or musculoskeletal radiology. Pediatric radiologists do a little bit of everything.
How did you connect with RP?
Our practice joined RP right before COVID, which turned out to be incredibly fortunate. The pandemic wreaked havoc on pretty much everybody, but we had support from RP. Being part of a radiology practice at RP’s scale versus a big local or even regional practice was helpful during the ups and downs. RP helped us see the bigger picture and supported us both financially and administratively, which was invaluable. Of course, we couldn’t have predicted COVID but joining when we did was a really lucky and positive move.
What excites you about RP? What is most fulfilling about working as a radiologist for RP?
What excites me about RP is its national presence. In pediatric radiology – and even across all radiology subspecialties – a common challenge is radiologists feeling like they don’t have a seat at the table. Before joining RP, we were already part of a large regional practice with a big presence in Austin and the surrounding metropolitan area, and it was a big step for us to join RP. But joining RP gave us something we didn’t have before: a true seat at the table. Whether it’s working with payors or hospital systems or leveraging organizational capabilities, RP brings support and infrastructure to bring everything together and move forward strategically and say, for example, “let’s invest in AI or this way of practice” or “let’s move away from this, because this isn’t working.” In a time when pediatric radiology – and medicine in general – is short-staffed at every level, having the ability to invest in the future and innovate is critical. RP makes that possible in a way most groups simply can’t.
You were recently named National Subspecialty Lead for Pediatric Radiology at RP. Tell us more about that role.
I’ve been on the national subspecialty advisory board for close to five years, and Dr. Rich Heller, Pediatric Radiologist and SVP of Health Policy at RP, encouraged me to get involved. The advisory board is a good platform for all subspecialties, but as a pediatric radiologist, it brings a small subgroup of people from larger groups to address shared challenges and offer subspecialty-focused resources, education and expertise available to other radiologists at RP. For example, if a radiologist without pediatric radiology expertise needs guidance or has a question, they can access specific content or reach out to one of us for support. As the lead, I get to help shape that direction, whether it’s deciding what content is important, bringing ideas to the group and collaborating with colleagues to make the information available to the rest of the practice. That kind of support is hard to find at smaller practices.
You’ve mentioned the collaborative environment you’ve experienced at RP. Tell us more about that.
The spirit of collaboration is a big part of what makes RP special. Personally, I’ve felt invited to the table, and the practice regularly encourages others to participate in forums and discussions. There are multiple platforms where radiologists can get involved. I’ve been encouraged to reach out to academic partners and participate in groups like the Society of Chiefs of Radiology at Children’s Hospitals. Several of us from RP are involved and having that presence gives us valuable face time at the academic level. It shows that pediatric radiologists in private practice are contributing meaningfully to the field, even if it’s not always through traditional academic research. It’s great to know how other groups operate, what challenges they face and how we might collaborate to solve shared problems. That kind of connection and problem-solving across practices is what makes this work so rewarding.
What does the future of radiology look like to you, and how will RP contribute to that?
Looking ahead, AI is going to be a huge part of radiology’s future. That’s where being part of a practice like RP matters. Like it or not, AI is here, and I’d rather be leading that change than chasing it. Being part of RP and being part of AI development gives us a seat at the table and lets us advocate for what matters most to us as physicians.
Dr. Shaheen Hussaini earned her medical degree from Aga Khan University Medical College in Karachi, Pakistan; completed her residency at the University of Arkansas for Medical Sciences in Little Rock, Arkansas; and completed her fellowship in pediatric imaging at Boston Children’s Hospital.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned radiology practice in the U.S. Learn more about our mission, values and practice principles at RadPartners.com. For the latest news from RP, follow along on our blog and on X, LinkedIn, Instagram and YouTube. Interested in learning about career opportunities? Visit our careers page.
A Patient (and Physician) Save: Dr. Dana Bonaminio’s Journey Through Breast Cancer
Dr. Dana Bonaminio, a breast radiologist in Nashville, has spent her career providing mammography care for women, promoting the importance of preventative care and early detection, and encouraging women to advocate for their breast health. But in 2024, she found herself on the other side of the conversation, facing the diagnosis of breast cancer herself.
Supplemental Screenings Led to Early Diagnoses
In addition to annual screening mammography, her own journey began after a routine supplemental breast MRI revealed suspicious masses in her left breast. Her care team followed up with a diagnostic mammogram and ultrasound, which confirmed four small masses correlating with the MRI findings. The following day, she underwent two ultrasound-guided biopsies.
“For me, the very worst part was the wait to learn about the tumor markers,” Dr. Bonaminio shared. She was scared, but hopeful. “I have two little kids,” she said.
The Power of Contrast-Enhanced Mammography
Despite a cancer diagnosis, her biopsy results brought a sense of relief. She learned she had favorable tumor markers and would not be required to have chemotherapy treatments, a stage one diagnosis. While she would need a bilateral mastectomy and reconstruction, there was hope she could avoid radiation if her lymph nodes and surgical margins were clear.
Before surgery, Dr. Bonaminio chose to have a contrast-enhanced mammogram. As a radiologist, she knew the power of contrast but seeing it as a patient was even more eye-opening. The contrast revealed cancers that conventional imaging had missed, hidden within her dense breast tissue.
“This technology could have caught my cancer earlier,” she said. “We need to ask why contrast-enhanced mammography isn’t offered as a screening tool. The answer should be yes, and we need to push for approval.”
After her bilateral mastectomies, she relied on her support system throughout her recovery. “It’s a solo battle, but I wasn’t alone,” she reflected. Ten days post-op, she received her final pathology results, and her recovery journey began.
Fueled to Advocate
Dr. Bonaminio leaned into advocacy after her reconstruction procedure. She participated in the Komen Walk in Nashville, attended the Pink Ribbon Good Gala in St. Louis and was honored at the Tennessee Titans Crucial Catch Game.
In early 2025, her experience led her to start a Pink Ribbon Good chapter in Nashville. The non-profit organization serves patients and their families affected by breast and gynecological cancer, offering free healthy meals, rides to treatment, housecleaning essentials and other support and resources.
At RP’s 2025 Practice Leadership Summit in Chicago, Dr. Bonaminio bravely shared her journey with her colleagues. RP radiologists and leaders joined RP CEO and Board Chair Rich Whitney and the practice in donating to support the Pink Ribbon Good Nashville Chapter, giving $30,000 to support the newly created organization. Later, in October, Pink Ribbon Good’s Nashville Chapter held its inaugural fundraising event “Ignite the Fight.”
Now, with the perspective of both physician and patient, Dr. Bonaminio is committed to advocacy. She said, “Whether it’s legislation for better access to care or supporting nonprofits that provide essential services, I’m excited for the rest of my career.”
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned radiology practice in the U.S. Learn more about our mission, values and practice principles at RadPartners.com. For the latest news from RP, follow along on our blog and on X, LinkedIn, Instagram and YouTube. Interested in learning about career opportunities? Visit our careers page.
Rad to Rad Learning: Male Breast Cancer
The Radiology Partners (RP) Breast Imaging National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
While male breast cancer is rare, it is often diagnosed at a later stage with poorer outcomes.
Male Breast Cancer
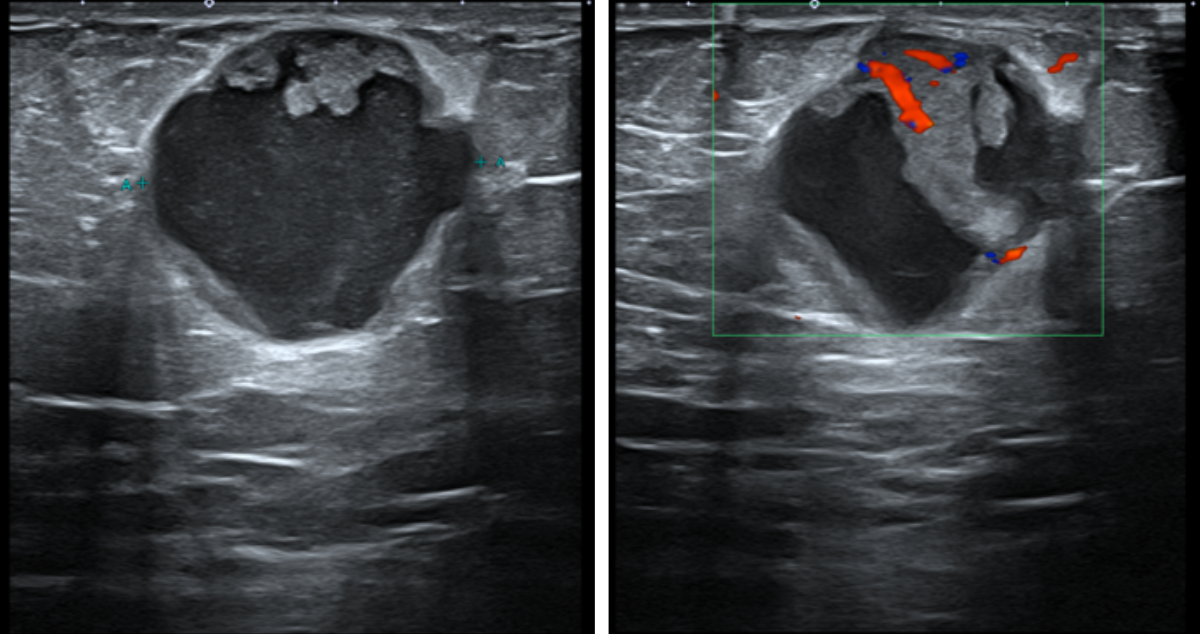
Most commonly found in the subareolar region, frequently with secondary signs including nipple retraction or thickening.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
Gynecomastia often presents as a retroareolar, flame-shaped density that gradually blends into the surrounding fat.
Can present with classic malignant features like spiculation or indistinct margins, but also as more benign-appearing oval or round shapes.
Any calcification should be considered suspicious.
US typically shows a hypoechoic solid mass with variable posterior acoustic properties and often increased vascularity on Doppler.
Always suspect malignancy if there is an irregular or spiculated retroareolar mass.
The Breast Imaging National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Rad to Rad Learning: Hyperechoic Breast Lesions
The Radiology Partners (RP) Breast Imaging National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
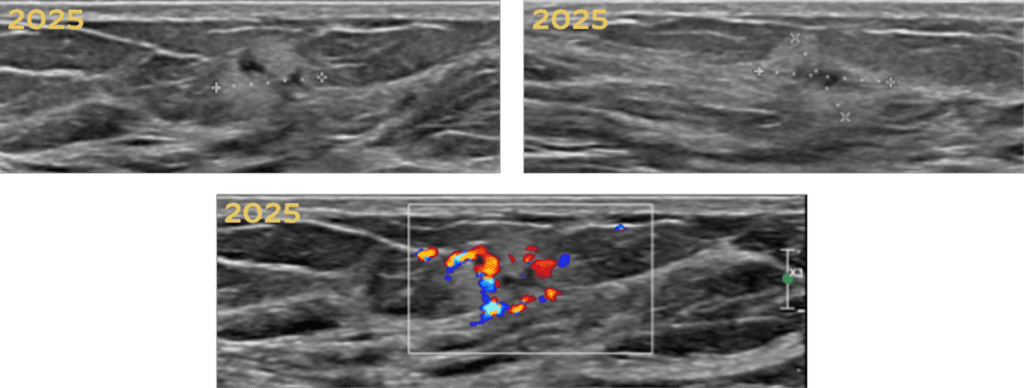
Hyperechogenicity is typically associated with benign breast lesions, including hamartoma, lipoma, angiolipoma, hemangioma, hematoma, fat necrosis, fibrosis, and galactocele. However, some rare malignant lesions may also appear hyperechoic.
Presents with palpable mass
Presents with new bruise
Hyperechoic Breast Lesions
Presents with persistent palpable concern
Biopsy-proven Invasive Lobular Carcinoma
Watch for subtle, suspicious features like irregular shape, non-circumscribed margins, non-parallel orientation, or posterior acoustic shadow.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
Don’t dismiss a lesion simply because it is hyperechoic. Correlate US findings with other modalities and the patient’s clinical history.
Consider specific histologies, not only invasive ductal or lobular carcinomas.
Rare cancers like angiosarcoma, lymphoma, and metastases can also present.
Don’t hesitate to recommend a biopsy for suspicious lesions. Do not rely solely on the hyperechoic appearance to rule out malignancy.
Contrast-enhanced mammography is a promising alternative for dense breasts.
Hyperechoic breast lesions are not always benign.
The Breast Imaging National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Why RP? A Q&A with Dr. Jean Weigert, Breast Radiologist
In honor of Breast Cancer Awareness Month, we spoke with Dr. Jean Weigert about the path that led her to become a breast radiologist, advocate for dense breast legislation and champion patient-centered care through decades of innovation.
Dr. Jean Weigert is a breast radiologist and breast imaging section chief at Jefferson Radiology, a Radiology Partners (RP)-affiliated practice. A Fellow of the American College of Radiology (FACR) and the Society of Breast Imaging (FSBI), she joined RP in 2017. Outside of work, Dr. Weigert’s passions include singing and ballroom dancing.
We talked to Dr. Weigert about her experience in the continually transforming field of breast imaging, her part in passing legislature in her home state of Connecticut and how the role of women has changed drastically in medicine.
What inspired you to be a radiologist?
I went to medical school in the late 1970s, when medicine still had quotas for women. Only about 20% of the class could be female. Most of us assumed we’d go into fields like pediatrics, OB-GYN or internal medicine. We didn’t think about surgery or what was then the “esoteric” field of radiology. I originally planned to pursue OB-GYN and took several electives, including one in radiology. During that rotation, I realized I could see anatomy in three dimensions. Not everyone can do that. The radiologists would show us images, and I could immediately recognize the structures. Everyone else was asking, “What are you seeing?”
Looking back, I think a lot of that came from my upbringing. I was raised in a very artistic home. My father was a physician who also painted, and we spent a lot of time in art museums. To me, the human body is beautiful, inside and out. Radiology let me appreciate it in a truly unique way. Unlike most people at the time, I went directly into radiology. I did a rotating internship and was fortunate to be accepted to some of the top residencies. I chose Columbia, and it was the right fit; their radiology department was excellent, and the experience shaped the rest of my career.
How did you become a breast radiologist?
Back when I trained, “breast imaging” didn’t really exist. But during my abdominal imaging fellowship, I started spending more time in gynecologic imaging and with early mammography, which was still developing in the early 1980s. At that time, mammograms were done on standard X-ray machines, often for women who already had a suspicious lump, as there was no screening yet.
After my training, I moved to Connecticut for my husband’s job. It was very hard to find a radiology position, especially as a woman. Ironically, I was hired by a group opening a mammography center, mainly because I was a woman and they thought it would be good for public relations. Reverse discrimination? Maybe. But I took the opportunity and ran with it, and that’s how I carved out a niche in breast imaging. I started teaching residents at the University of Connecticut once a month, hauling in my mammograms in a bag. They called me the “bag lady.” Over time, I built a reputation as a women’s imager, doing research, lecturing and growing the practice in ways no one else was really doing.
What was mammography like for women in the 1980s?
It was a very different world. Women typically came in because they felt a lump. Cancers were larger and often already metastatic. We didn’t have minimally invasive biopsies; surgeons would remove large pieces of tissue. If the pathology came back as cancer, the woman would often wake up having had a mastectomy. Lumpectomies weren’t a thing yet. We’ve come a long way, but even today, we still see too many advanced cancers. We all hoped we’d catch every cancer early – under 1 cm – but that’s not always the case. Still, with the tools we have now, we can detect more cancers earlier than ever before.
What do you wish more women knew about breast health today?
That they have power and control over their health. I say this to patients all the time: “You know your body better than anyone. If something doesn’t feel right, don’t ignore it.” Even if it turns out to be nothing, that’s still a win. We’re also seeing a troubling trend, with more aggressive breast cancers in younger women. I’ve seen women in their 20s with invasive disease. Since screening usually starts at 40, these cancers are often only found because the patient noticed a lump. That’s why self-awareness and risk-based screening are so important.
Speaking of guideline, what should women understand beyond “get a mammogram at 40”?
Guidelines are just that – guidelines. If you have a first-degree relative with breast cancer, you should start screening 10 years earlier than their age at diagnosis. And now we have genetic risk models and tools to assess a woman’s lifetime risk. But I also remind patients: “Don’t say you’re not at risk just because you have no family history. If you have breasts, you’re at risk.”
What innovations have transformed breast imaging during your career?
When I started, mammograms were done on film and developed in dark rooms. Fast-forward to today, and we have:
Digital mammography, which allows real-time manipulation of images.
Tomosynthesis (3D mammography), which gives us millimeter-thin slices of breast tissue—like a CT scan of the breast.
Advanced ultrasound, which can evaluate vascularity and tissue characteristics.
MRI, now a powerful tool for high-risk women, with sequences that reveal solid vs. cystic lesions and vascular kinetics.
Contrast-enhanced mammography and molecular imaging, which give us insight into metabolic activity—cancers are often hypermetabolic.
AI, which helps us assess density, flag subtle findings and improve accuracy.
We’ve gone from “how did we even find cancers back then?” to having an array of incredible tools today. The challenge now is interpreting all that data responsibly and minimizing unnecessary biopsies while still catching early, aggressive cancers.
You played a role in passing Connecticut’s dense breast legislation. Can you tell us more about that?
In 2005, Connecticut passed a little-known law allowing ultrasounds for women with dense breasts, but no one was using it. Then a close colleague of mine was diagnosed with Stage III breast cancer shortly after receiving a “normal” mammogram. Her breasts were dense, and the mammogram had missed it. She became a tireless advocate. Together with the Connecticut Radiology Society, we lobbied to make breast density reporting and supplemental screening the standard. In 2009, Governor Rell, herself a survivor, signed the first dense breast law in the U.S.
I also led some of the earliest studies on screening ultrasound, publishing papers that showed we could detect an additional 3–4 cancers per 1,000 women. That’s huge. Now, 38 states have laws, and as of September 2024, every woman in the U.S. must be notified of her breast density on her mammogram results.
What’s been the most meaningful part of working with patients?
It’s the human part of radiology. When I can tell a woman, “This looks totally fine,” and she hugs me in relief—it’s amazing. When I have to tell a patient we need a biopsy, I’m honest and compassionate. I say, “I’ve been doing this long enough to know that when I don’t know what something is, I need to find out.” Then I lay out the plan. Patients appreciate that clarity.
You’re now part of Jefferson Radiology and RP. How has that experience been?
What drew me to Jefferson Radiology was their subspecialty model, where I could focus on what I do best. The volume, the team and the technology elevated my skills. Honestly, it felt like a mini fellowship. I learned so much from my colleagues. Radiology has changed drastically over my career and so has the role of women in medicine.
As part of RP, I’ve gotten to participate in exciting national projects, like research on breast calcifications. That level of collaboration didn’t happen in my smaller group before. I also appreciate RP’s openness to innovation and the fact that they’ve created a platform for clinical voices like mine to be heard.
What honors have shaped your career?
In 2008, I became a Fellow of the American College of Radiology (FACR) an honor given to only 10% of radiologists, and even fewer women at the time. I was also appointed chair of the ACR Accreditation Committee for Mammography and continue to serve as a senior reviewer for MQSA.
In 2020, I was honored to become a Fellow of the Society of Breast Imaging (FSBI). Most SBI fellows are academics with dozens of publications. I’ve always been a clinician, a “closet academic.” They actually adjusted the criteria to allow recognition of clinical excellence—and I was the first to be awarded through that path.
How do you spend your time outside of medicine?
I have five daughters—two of my own and three stepdaughters—and seven grandchildren. I’m not the “babysitting grandma,” but I’m very involved. Some of my daughters now get mammograms, and I’m proud they take their health seriously—even if they sometimes forget to tell me!
Outside of family, I have two big passions: singing and competitive ballroom dancing. I’ve been dancing for 30 years. It’s great for my body and my brain and it forces me to let someone else lead, which isn’t easy for me! I also love history and genealogy. I come from a long line of scientists and physicians, including a Nobel Prize winner, in some ways, this path was always part of my DNA.
Dr. Jean Weigert earned her medical degree from State University of New York Upstate Medical Center, and she completed both her fellowship in abdominal imaging and residency in diagnostic radiology at Columbia-Presbyterian Medical Center.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned radiology practice in the U.S. Learn more about our mission, values and practice principles at RadPartners.com. For the latest news from RP, follow along on our blog and on X, LinkedIn, Instagram and YouTube. Interested in learning about career opportunities? Visit our careers page.
Radiology Partners Launches AI-Enabled Clinical Program to Advance Women’s Preventative Health
Mammo Enhance Heart™ offers two-in-one screening for breast cancer and cardiovascular disease risk
(NASHVILLE, Tenn.) Oct. 2, 2025 — Radiology Partners (RP), the leading provider of technology-enabled radiology services in the U.S., today announced the launch of Mammo Enhance Heart™, an AI-enabled clinical program designed to redefine preventive care for women. The program supports early detection and risk stratification by identifying breast arterial calcifications (BAC), a marker linked to cardiovascular disease using screening mammograms and coordinating follow-up with a local network of cardiologists. Mammo Enhance Heart™ is currently available at Desert Radiology, an RP-affiliated practice, with plans to expand to additional markets in the near term.
The Mammo Enhance Heart™ program utilizes an FDA-cleared AI tool to detect the presence of BAC, buildup of calcium in the breast arteries, during a woman’s regular mammogram screening. An internally developed risk-scoring methodology stratifies patients by likely cardiovascular risk, and program personnel coordinate follow-up for higher-risk patients through a locally developed network of cardiology specialists. Follow-up data are also utilized to continuously refine risk prediction and care protocols. Early detection of BAC helps identify cardiovascular risk in women who might otherwise remain undiagnosed until more serious symptoms emerge. Incorporating the Mammo Enhance Heart™ program into annual screening mammograms provides valuable insights into a patient’s long-term health risks, ensures appropriate clinical follow-up and reduces the need for additional exams or radiation exposure.
“Cardiovascular disease is the leading cause of death among women in the U.S., and women with BAC are approximately 51% more likely to develop heart disease or stroke,” said Dr. Arthy Saravanan, Breast Radiologist and Associate Chief Medical Officer for Radiology Partners. “Mammo Enhance Heart™ is a revolutionary program for women’s healthcare, improving detection, incorporating risk assessment and empowering women to take control of their health. Mammo Enhance Heart™ presents a significant step forward not only in preventive healthcare, but also in the overall patient experience.”
The Mammo Enhance Heart™ program utilizes AI to analyze a patient’s mammogram to determine the presence, absence and location of BAC. Following completion of the exam, expert radiologists review the results to confirm any findings and determine a risk score. The exam results and risk score are shared directly with the patient and their provider along with appropriate follow-up recommendations, helping providers tailor care pathways and engage cardiology teams when needed. Patients identified with BAC may be candidates for additional clinical evaluation of general health. Patients requiring cardiologist consultation may choose from a network of local cardiologists trained on the clinical objectives of Mammo Enhance Heart™.
“Integrating this screening into routine mammogram appointments allows providers to monitor changes over time without additional exams,” Dr. Saravanan added. “With this continuous evaluation, patients are more in tune with their risk factors and overall health, making this a powerful program for managing long-term health.”
Already live at Desert Radiology, RP plans to expand Mammo Enhance Heart™ to additional markets throughout 2025 and 2026.
About Radiology Partners
Radiology Partners, through its affiliated practices, is the leading technology-enabled radiology practice in the U.S., serving more than 3,400 hospitals and other healthcare facilities with high quality radiology, technology and artificial intelligence solutions. As a physician-led and physician-owned practice, our mission is to transform radiology by innovating across clinical value, technology, service and economics, while elevating the role of radiology and radiologists in healthcare. Using a proven healthcare services model, Radiology Partners provides consistent, high-quality care to patients, while delivering enhanced value to the hospitals, clinics, imaging centers and referring physicians we serve. Learn more at radpartners.com and connect with us on LinkedIn, X, Instagram and YouTube.
Rad to Rad Learning: False Negative in Dense Breast
The Radiology Partners (RP) Breast Imaging National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
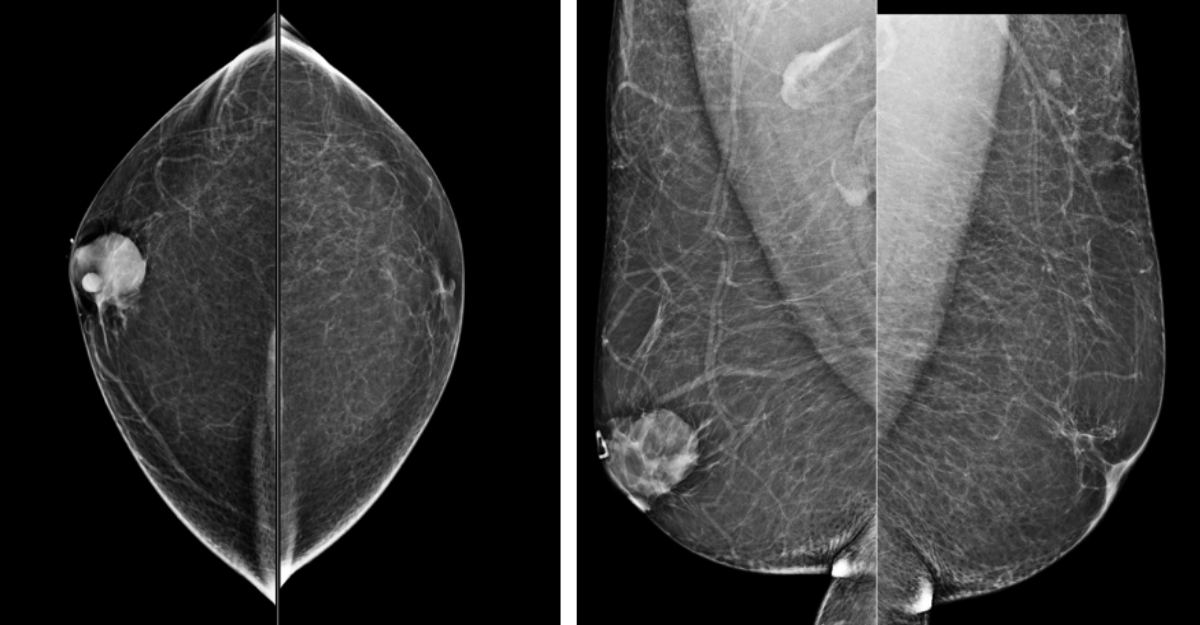
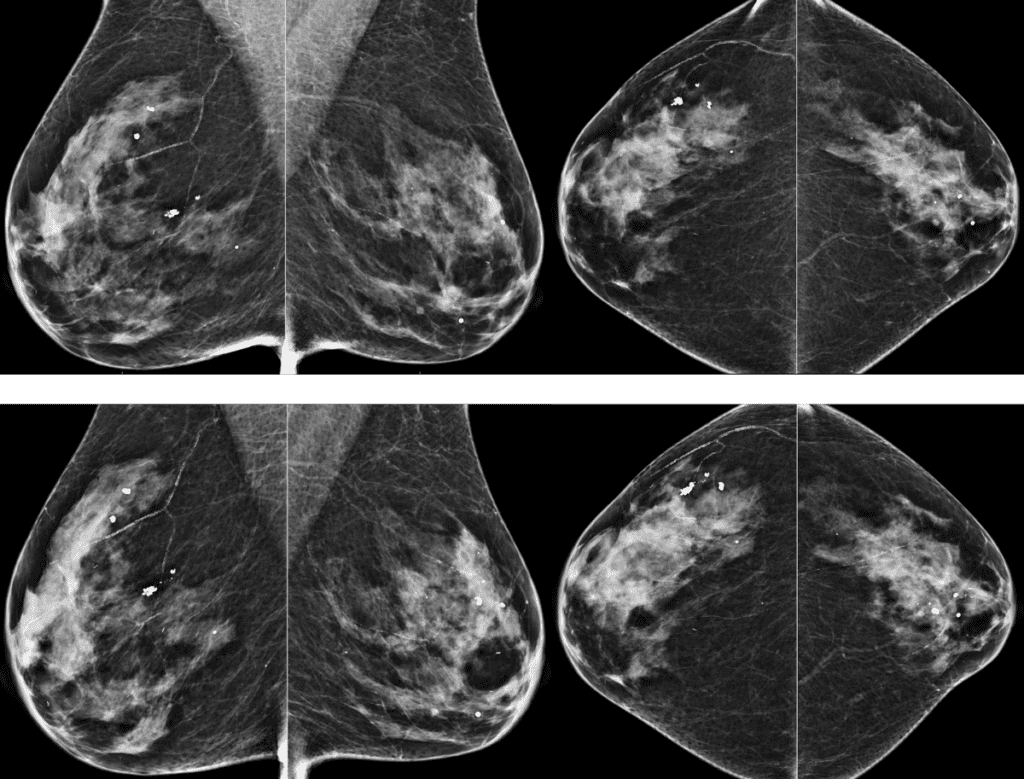
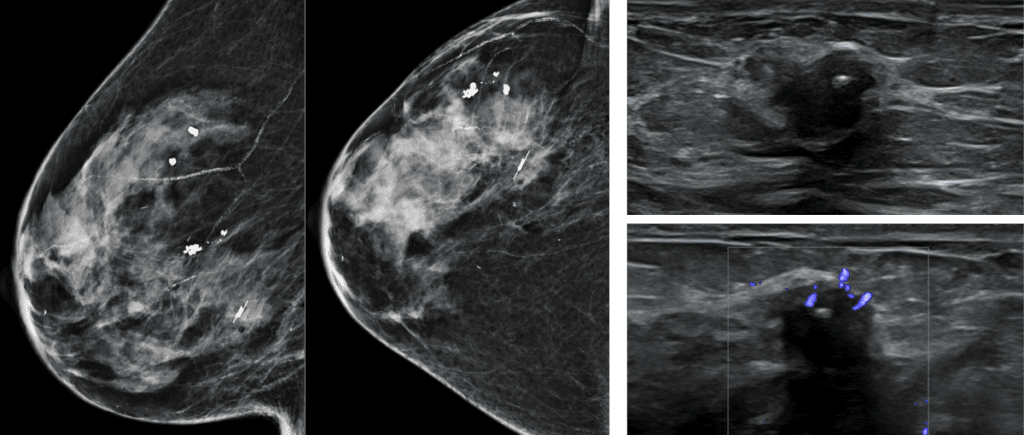
Mammographic sensitivity can drop to as low as 50% in extremely dense breasts (Category D), compared to nearly 90% in fatty breasts (Category A).
Top: Screening 2021, Bottom: Screening 2024
False Negative in Dense Breast
Cancers detected by supplemental screening whole-breast ultrasound are often invasive, however small and node negative, indicating they are found at an early, more treatable stage.
Post-biopsy reflector. Right breast, 7:00.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
Breast density is an interdependent risk factor for breast cancer.
Supplemental breast ultrasound can detect an additional 2-4 cancers per 1,000 women screened with dense breasts.
Ultrasounds have a high false positive rate. The positive predictive value is 5-10% (compared to 25-40% for mammography).
Women with dense breasts and other risk factors (e.g., strong family history, genetic mutations) may benefit most from supplemental MRI.
Contrast-enhanced mammography is a promising alternative for dense breasts.
In dense breasts, US can find additional clinically significant cancers.
The Breast Imaging National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Rad to Rad Learning: Incidental Intra-Cardiac Lesions
The Radiology Partners (RP) Cardiothoracic Imaging National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
Although infrequent, intra-cardiac thrombi or masses have significant ramifications and can result in pulmonary or systemic embolization.
Incidental Intra-Cardiac Lesions
All three images are from CT abdomen/pelvis exams.
1. Left atrial appendage thrombus
2. Right artial mass.
3. Left ventricular mass.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
Though motion artifacts and contrast flow artifacts can make the heart chambers difficult to assess, include them in your search patterns of non-cardiac examinations.
Think beyond heart size and coronary calcifications when reviewing the heart.
The Cardiothoracic Imaging National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.


 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
 Multiphase CTA = Faster, more specific, better anatomic localization.
Multiphase CTA = Faster, more specific, better anatomic localization.




 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.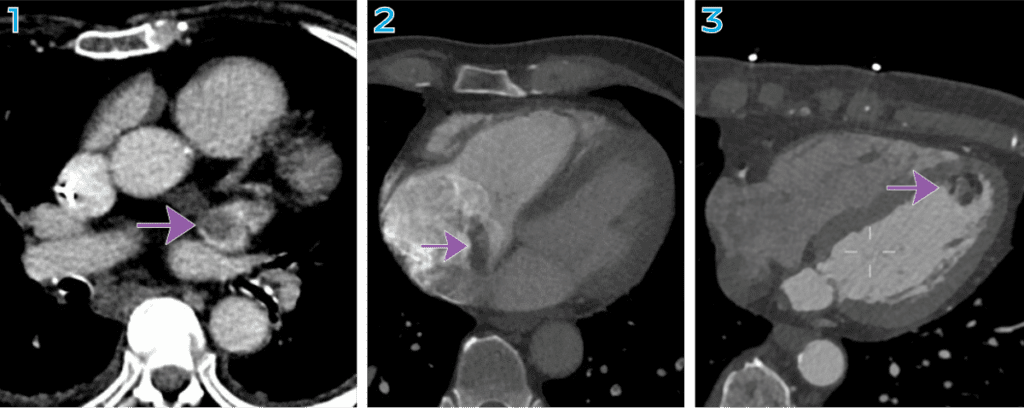 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.