Rad to Rad Learning: Three-Phase Bone Scan: Prosthesis Evaluation
The Radiology Partners (RP) NMMI Radiology National Subspecialty Division (NSD)presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
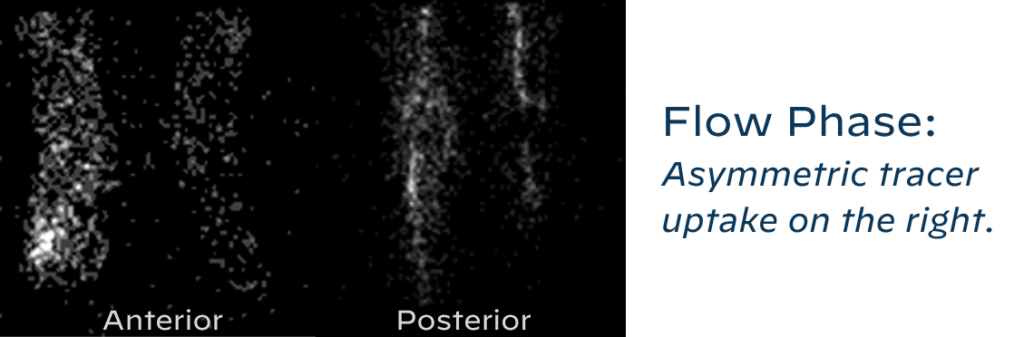
Diagnosis of prosthetic loosening (septic or aseptic) can be achieved with three-phase bone scan using proper technique and specific scintigraphic findings.
63/yo F with right knee pain, bilateral TKAs in 2010
Flow Phase: Asymmetric tracer uptake on the right.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
Time since surgery is important history. Patients can have reactive uptake on all three phases up to 1-2 years since surgery.
Cemented prostheses usually revert to baseline uptake after one year. Non-cemented prostheses can take up to two years.
Laterality and site of pain are also essential history that increase the diagnostic yield.
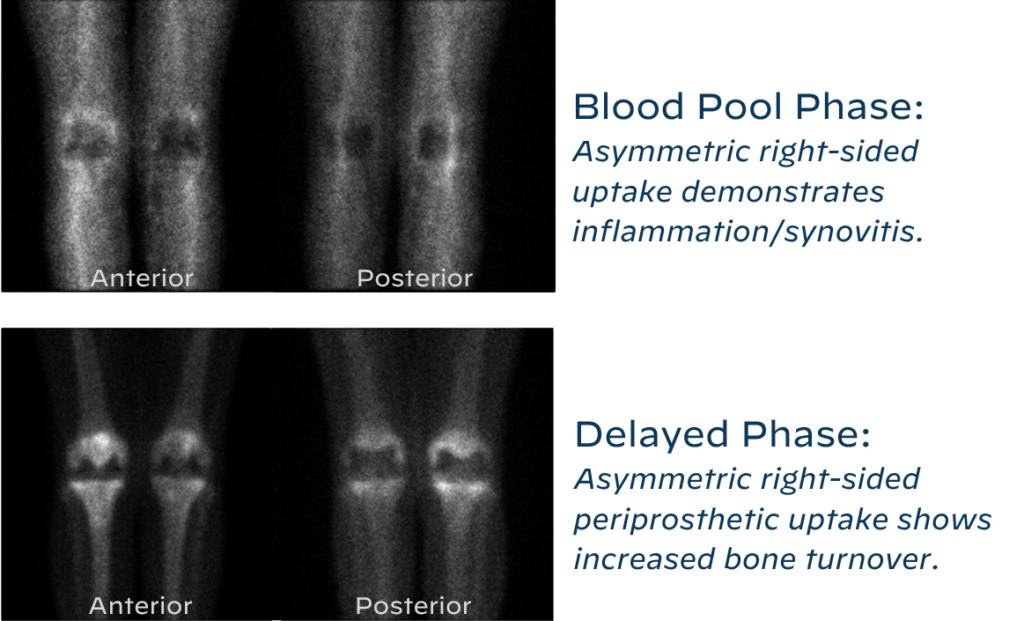
Takeaway: Abnormal uptake in all three phases likely indicates septic loosening.
The The NMMI Radiology National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Rad to Rad Learning: Anterior Pneumothorax
The Radiology Partners (RP) Pediatric Radiology National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
This condition is associated with high morbidity but is difficult to see on supine neonates.
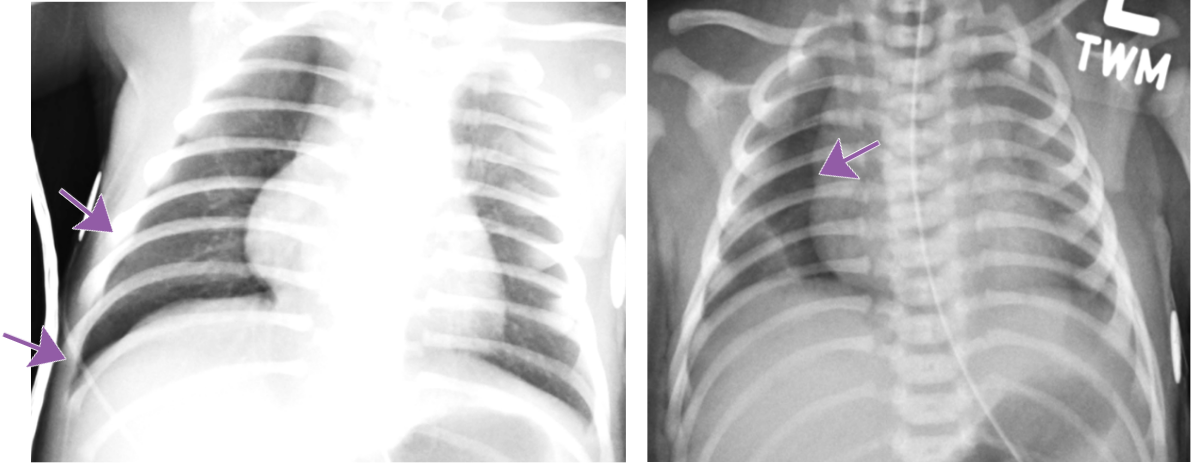
Anterior Pneumothorax
Hallmarks: Deep sulcus sign, no lung marking at the edge of right lung, increased sharpness of the cardiomediastinal border, more prominent on expiration.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
May be bilateral.
Can occur in both term and preterm babies.
Compare lung lucency between both sides.
Decubitus radiograph can be a helpful tool for confirmation.
Takeaway: Even a suspected pneumothorax is a critical result and should be called.
The Pediatric Radiology National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Rad to Rad Learning: Slipped Capital Femoral Epiphysis
The Radiology Partners (RP) Pediatric Radiology National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
Slipped Capital Femoral Epiphysis (SCFE) is a common and urgent diagnosis and needs to be communicated with the referring provider.
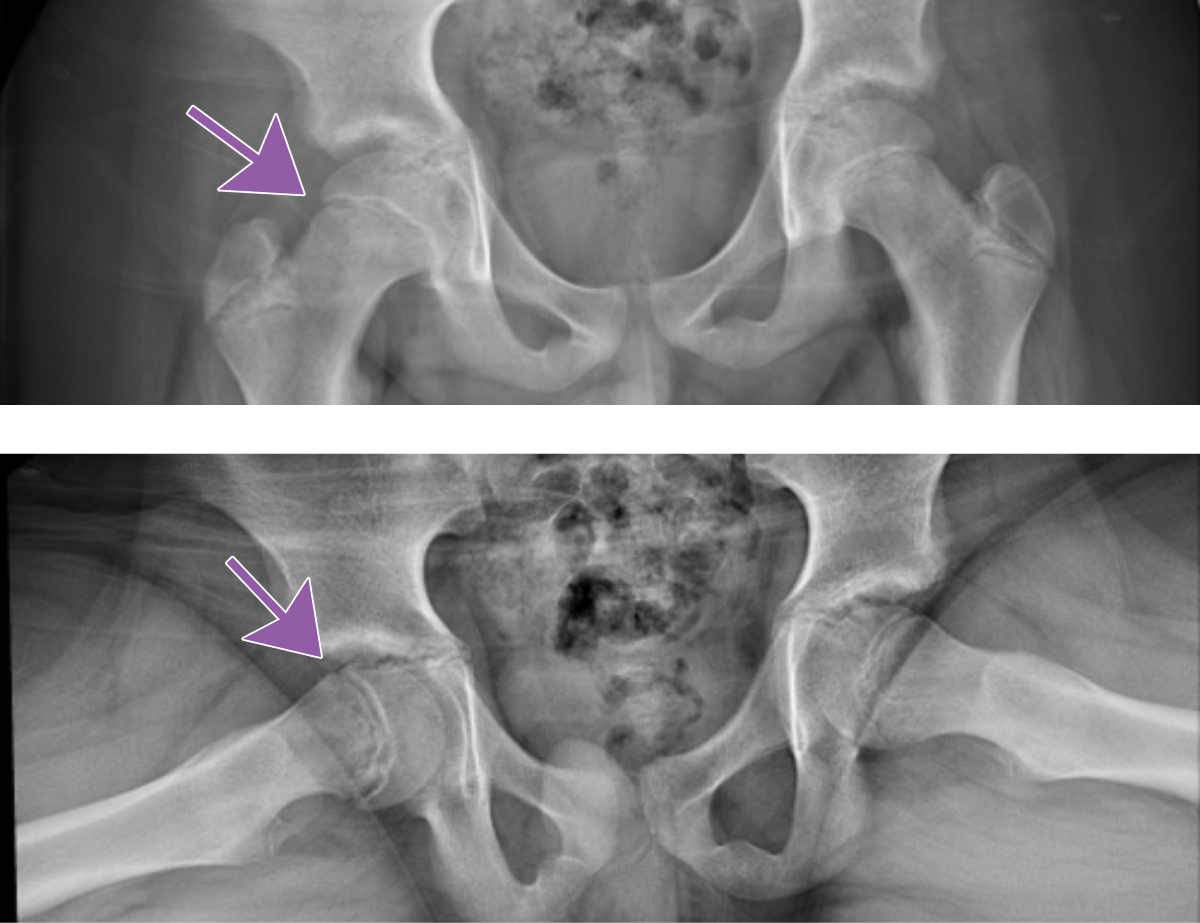
Slipped Capital Femoral Epiphysis
Note the medial and posterior displacement of the right femoral head and widened physis. Frog lateral views are generally more sensitive.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
Commonly missed diagnosis that leads to increased complications.
Complications include osteonecrosis, chondrolysis, chronic pain, and growth arrest.
Having a high index of suspicion is helpful.
For at-risk patients, compare the hips on both views.
Takeaway: Make sure to communicate positive findings to the referring provider.
The Pediatric Radiology National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Why RP? A Q&A with Dr. Shaheen Hussaini, Pediatric Radiologist
Dr. Shaheen Hussaini discusses how Radiology Partners (RP) offers resources, support, collaboration and innovation to empower radiologists to make a meaningful impact on patient care and the future of radiology.
Dr. Shaheen Hussaini is the National Subspecialty Lead (NSL) for Pediatric Radiology at RP. A pediatric radiologist at Austin Radiological Association (ARA), she and her practice joined RP in 2019. She is a member of the American College of Radiology, Radiological Society of North America, Society of Pediatric Radiology and Texas Medical Association. Outside of work, she enjoys traveling and spending time with her husband and children, and she loves reading, hiking and trying new activities – often bringing her family along for the adventure.
We talked to Dr. Hussaini about her role as NSL for Pediatric Radiology and how RP offers radiologists a true seat at the table.
Tell us about why you chose radiology and, ultimately, pediatric radiology.
What interested me in radiology was how collaborative it is. You get to talk to a variety of physicians and sub-specialists and use those different perspectives to determine the best way to answer their questions about the patient. It’s also fun to play with toys – and radiology has a lot of toys. In pediatric radiology, you interact with patients who don’t have a voice; these are small patients often too young to explain what’s wrong. It helps that they’re cute, even when they’re angry at you because what you’re doing to them is not fun. Going through pediatric radiology training while pregnant and as a new parent helped me relate to the children and families in a much more personal way. It elicited a desire to help and play small part of their diagnostic and treatment journey, and I felt I could be more empathetic and understanding. Another thing I love about pediatric radiology is the variety, because there are all varying subspecialties that are part of pediatric radiology instead of focusing on just one area, such as neuroradiology or musculoskeletal radiology. Pediatric radiologists do a little bit of everything.
How did you connect with RP?
Our practice joined RP right before COVID, which turned out to be incredibly fortunate. The pandemic wreaked havoc on pretty much everybody, but we had support from RP. Being part of a radiology practice at RP’s scale versus a big local or even regional practice was helpful during the ups and downs. RP helped us see the bigger picture and supported us both financially and administratively, which was invaluable. Of course, we couldn’t have predicted COVID but joining when we did was a really lucky and positive move.
What excites you about RP? What is most fulfilling about working as a radiologist for RP?
What excites me about RP is its national presence. In pediatric radiology – and even across all radiology subspecialties – a common challenge is radiologists feeling like they don’t have a seat at the table. Before joining RP, we were already part of a large regional practice with a big presence in Austin and the surrounding metropolitan area, and it was a big step for us to join RP. But joining RP gave us something we didn’t have before: a true seat at the table. Whether it’s working with payors or hospital systems or leveraging organizational capabilities, RP brings support and infrastructure to bring everything together and move forward strategically and say, for example, “let’s invest in AI or this way of practice” or “let’s move away from this, because this isn’t working.” In a time when pediatric radiology – and medicine in general – is short-staffed at every level, having the ability to invest in the future and innovate is critical. RP makes that possible in a way most groups simply can’t.
You were recently named National Subspecialty Lead for Pediatric Radiology at RP. Tell us more about that role.
I’ve been on the national subspecialty advisory board for close to five years, and Dr. Rich Heller, Pediatric Radiologist and SVP of Health Policy at RP, encouraged me to get involved. The advisory board is a good platform for all subspecialties, but as a pediatric radiologist, it brings a small subgroup of people from larger groups to address shared challenges and offer subspecialty-focused resources, education and expertise available to other radiologists at RP. For example, if a radiologist without pediatric radiology expertise needs guidance or has a question, they can access specific content or reach out to one of us for support. As the lead, I get to help shape that direction, whether it’s deciding what content is important, bringing ideas to the group and collaborating with colleagues to make the information available to the rest of the practice. That kind of support is hard to find at smaller practices.
You’ve mentioned the collaborative environment you’ve experienced at RP. Tell us more about that.
The spirit of collaboration is a big part of what makes RP special. Personally, I’ve felt invited to the table, and the practice regularly encourages others to participate in forums and discussions. There are multiple platforms where radiologists can get involved. I’ve been encouraged to reach out to academic partners and participate in groups like the Society of Chiefs of Radiology at Children’s Hospitals. Several of us from RP are involved and having that presence gives us valuable face time at the academic level. It shows that pediatric radiologists in private practice are contributing meaningfully to the field, even if it’s not always through traditional academic research. It’s great to know how other groups operate, what challenges they face and how we might collaborate to solve shared problems. That kind of connection and problem-solving across practices is what makes this work so rewarding.
What does the future of radiology look like to you, and how will RP contribute to that?
Looking ahead, AI is going to be a huge part of radiology’s future. That’s where being part of a practice like RP matters. Like it or not, AI is here, and I’d rather be leading that change than chasing it. Being part of RP and being part of AI development gives us a seat at the table and lets us advocate for what matters most to us as physicians.
Dr. Shaheen Hussaini earned her medical degree from Aga Khan University Medical College in Karachi, Pakistan; completed her residency at the University of Arkansas for Medical Sciences in Little Rock, Arkansas; and completed her fellowship in pediatric imaging at Boston Children’s Hospital.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned radiology practice in the U.S. Learn more about our mission, values and practice principles at RadPartners.com. For the latest news from RP, follow along on our blog and on X, LinkedIn, Instagram and YouTube. Interested in learning about career opportunities? Visit our careers page.
Rad to Rad Learning: Incidental Intra-Cardiac Lesions
The Radiology Partners (RP) Cardiothoracic Imaging National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
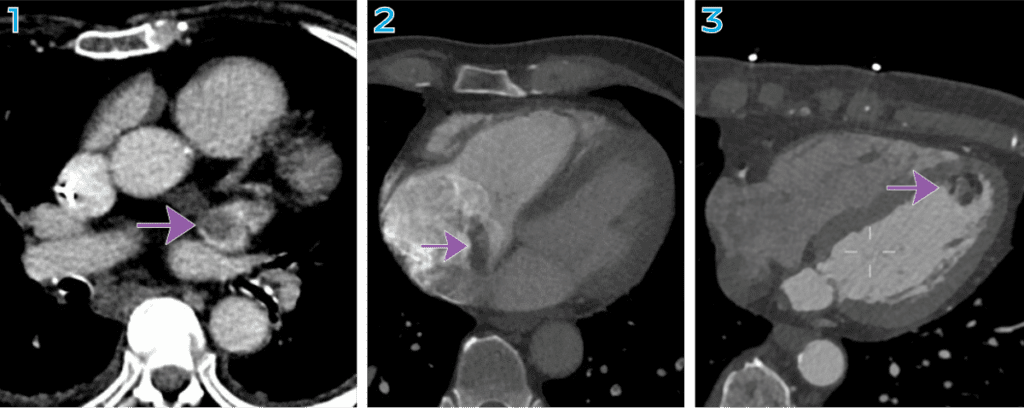
Although infrequent, intra-cardiac thrombi or masses have significant ramifications and can result in pulmonary or systemic embolization.
Incidental Intra-Cardiac Lesions
All three images are from CT abdomen/pelvis exams.
1. Left atrial appendage thrombus
2. Right artial mass.
3. Left ventricular mass.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights
Though motion artifacts and contrast flow artifacts can make the heart chambers difficult to assess, include them in your search patterns of non-cardiac examinations.
Think beyond heart size and coronary calcifications when reviewing the heart.
The Cardiothoracic Imaging National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Rad to Rad Learning: Ileocolic vs. Small Bowel Intussesception
The Radiology Partners (RP) Pediatric Radiology National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
Small bowel intussusceptions do not typically require management but can be mistaken for the urgent diagnosis of ileocolic intussusception.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
If uncertain, another scan can be obtained in ~30 minutes.
<2cm LLQ intussusceptions are likely physiologic. If uncertain, reassess.
The Pediatric Radiology National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Rad to Rad Learning: Pyloric Stenosis
The Radiology Partners (RP) Pediatric Radiology National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
The Pediatric Radiology NSD is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice.
Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Rad to Rad Learning: Childhood Appendicitis
The Radiology Partners (RP) Pediatric Radiology National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
The Pediatric Radiology NSD is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice.
Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Rad to Rad Learning: Abusive Head Injury
The Radiology Partners (RP) Pediatric Radiology National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
ThePediatric Radiology NSD is part of RP’s Clinical Value Team, whichworks to elevate patient care and enhance value through innovation, collaboration and education.To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what weencounter in our day-to-day practice.
Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.
Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Clinical Pathway: RP’s Clinical Value Team presents best practices for neonatal urinary tract dilation
Radiology Partners (RP) recently created a Neonatal Urinary Tract Dilation Clinical Pathway.
Dr. Rich Heller leads RP’s NSD for pediatric radiology. In partnership with an advisory board of practicing pediatric radiologists, he spearheads the development and implementation of programs with a mission to enhance clinical value and quality in pediatric radiology across RP. The NSD focuses on refining best practice recommendations, advancing image quality and patient services and aligning with the most current industry standards. They share these resources throughout RP so that all practices can deliver high-quality subspecialty care to patients in their communities.
“We are excited to announce this program for our radiologists,” Dr. Heller said. “The UTD classification system was developed by representatives from multiple stakeholder societies and creates a standardized approach to evaluating the pediatric kidney and communicating the findings to the referring care team, helping improve patient care.”
Radiology Partners Clinical Value Team exists to elevate patient care and enhance value through innovation, collaboration and education. Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
Nguyen HT, Benson CB, Bromley B, Campbell JB, Chow J, Coleman B, Cooper C, Crino J, Darge K, Herndon CD, Odibo AO, Somers MJ, Stein DR. Multidisciplinary consensus on the classification of prenatal and postnatal urinary tract dilation (UTD classification system). J Pediatr Urol. 2014 Dec;10(6):982-98. doi: 10.1016/j.jpurol.2014.10.002. Epub 2014 Nov 15. PMID: 25435247.


 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
 Takeaway: Abnormal uptake in all three phases likely indicates septic loosening.
Takeaway: Abnormal uptake in all three phases likely indicates septic loosening.

 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.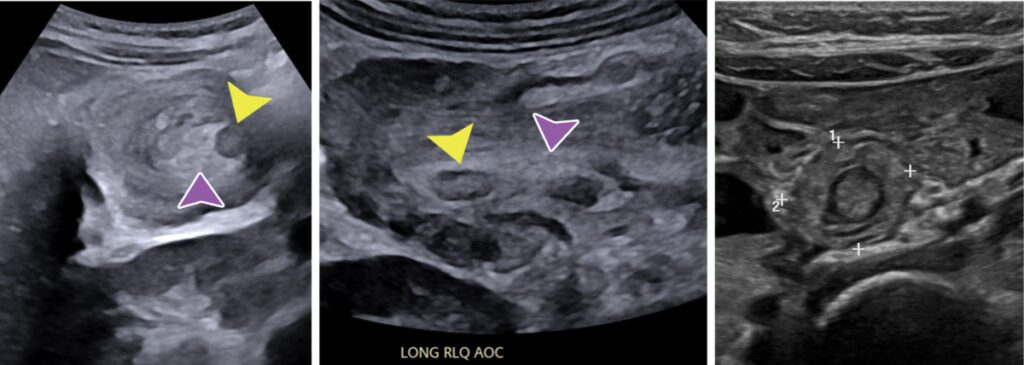 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived. Visit the
Visit the 
 Visit the
Visit the 