
The Radiology Partners (RP) Pediatric Radiology National Subspecialty Division (NSD) presents our newest Rad to Rad Learning case.
Peer Learning Opportunity
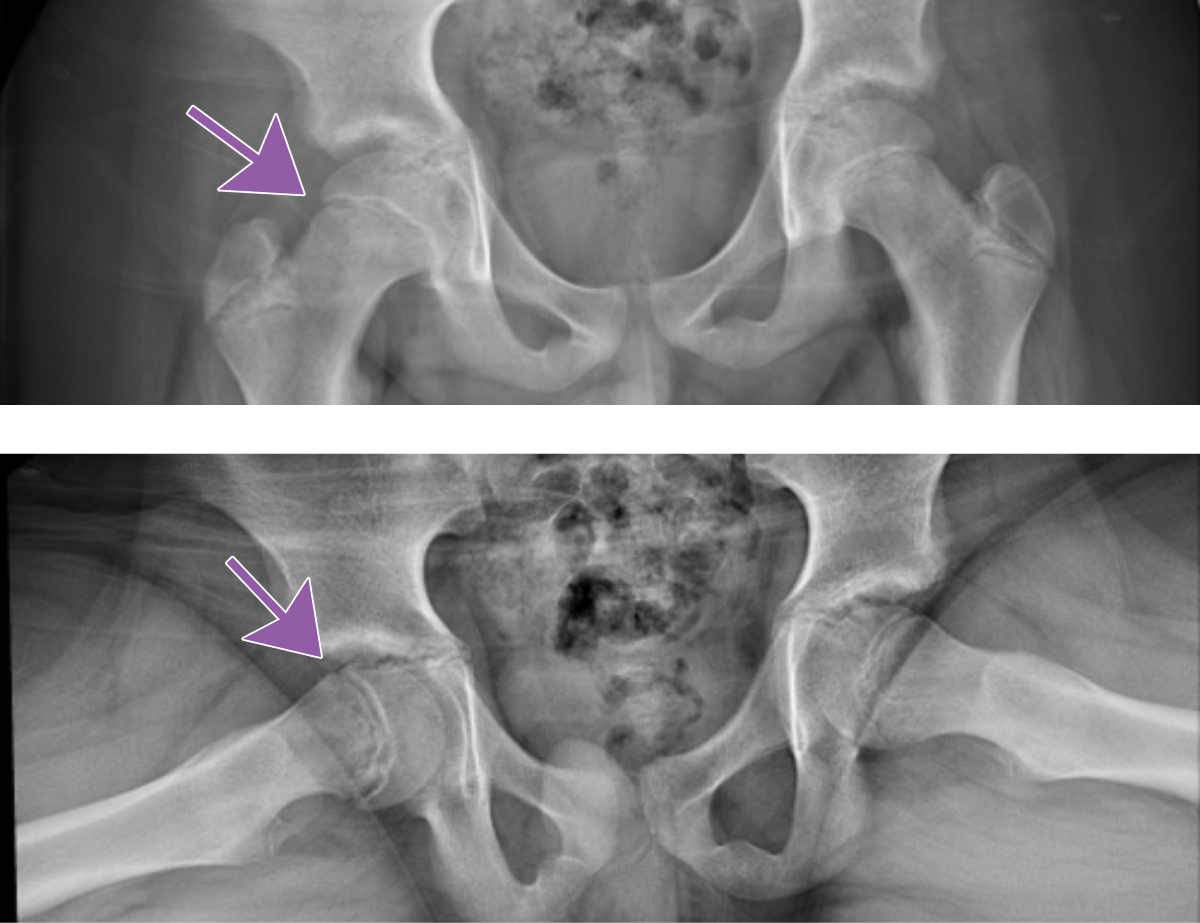
Slipped Capital Femoral Epiphysis (SCFE) is a common and urgent diagnosis and needs to be communicated with the referring provider.
Slipped Capital Femoral Epiphysis

Note the medial and posterior displacement of the right femoral head and widened physis. Frog lateral views are generally more sensitive.
 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Practical Insights 
-
-
Commonly missed diagnosis that leads to increased complications.
-
Complications include osteonecrosis, chondrolysis, chronic pain, and growth arrest.
-
Having a high index of suspicion is helpful.
-
For at-risk patients, compare the hips on both views.
-
 Takeaway: Make sure to communicate positive findings to the referring provider.
Takeaway: Make sure to communicate positive findings to the referring provider.
The Pediatric Radiology National Subspecialty Division (NSD) is part of RP’s Clinical Value Team, which works to elevate patient care and enhance value through innovation, collaboration and education. To advance this goal, our radiologists and advanced practice providers are committed to sharing peer learning as valuable reminders and insights about what we encounter in our day-to-day practice. Check back here and on X, LinkedIn and Instagram to see these common cases and our findings.
Visit the Clinical Resources page for more cases and to see what we’ve developed to enhance best practice recommendations, elevate image quality and patient care and update current standards throughout RP’s network of practices, all to deliver excellent radiology services to patients, referring clinicians and client partners.

Radiology Partners, through its owned and affiliated practices, is a leading physician-led and physician-owned technology-enabled radiology practice in the U.S. For the latest news from RP, follow us on X, LinkedIn, Instagram, YouTube and the blog.
 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived. Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived. Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived. Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
 Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.
Shared to improve patient safety and healthcare delivery in the provision of radiology services. The circumstances and facts are changed, altered, or deidentified to preserve confidentiality. Privileges have not been waived.